“Photobiology is a scientific field involving biology, physics, and chemistry that studies the effects of optical radiation on living organisms.”
“Lighting systems are artificial sources of optical radiation used primarily to provide light to the eyes for performing visual processes in the absence of sufficient natural light.”
The primary photobiological effect of visible light sources is vision. In humans, light interacts with certain ocular tissues and types of retinal photoreceptors (cones, rods, optic neurons, etc.) to send received signals to the retinal visual nerve network, which is directly connected to the brain via optic nerves, helping us perceive light and images. However, because of this exposure to light, if we do not control it (in terms of intensity or exposure time), photobiological impacts can affect human health.
Beyond vision, one of the most important photobiological impacts of visible light on animals is the regulation of circadian rhythms. This effect has been observed and studied by biologists in humans (including some blind subjects) and many other animal species since the 1980s. Light is the most powerful agent for the daily synchronization of the biological clock, which inherently operates on a cycle of approximately 24 hours (varying by a few to several dozen minutes).
In the absence of light stimuli, the biological clock drifts and becomes desynchronized from daily schedules. The most notable feature of this synchronization mechanism is that it occurs only through the eyes. The discovery of a new type of photoreceptor cell in the retina in the 1990s provided the physiological basis to explain this phenomenon. A small number of ganglion cells were found to be photosensitive without contributing to vision. It has been proven that the optical stimulation of these cells is responsible for suppressing the production of melatonin—the sleep hormone—and is also the cause of many other non-visual effects such as pupil constriction, increased heart rate, elevated body temperature, etc.
“Photobiological safety” refers to the undesirable effects of optical radiation on human tissues, specifically the skin and the eyes. These impacts can stem from several causes, such as the type of tissue exposed, the wavelength of the incident radiation, the intensity of exposure, and the duration of exposure. Depending on these parameters, effects can be temporary (reversible) or permanent in cases of severe exposure.
I. PROBLEM STATEMENT
Light affects the human body through two mechanisms:
- Direct: Absorption through the body’s cells.
- Indirect: Through hormones in the blood or chemical signals released from the body’s neurons.
Sunlight is considered to provide “Full Spectrum light.” When reading or working under this light, human eyes are at their healthiest as they do not need to perform additional adjustments. However, depending on intensity and exposure time, sunlight can also harm our skin, causing sunburn, darkening, itching, etc., or affect the eyes, leading to glare, dazzle, keratitis, pinguecula, pterygium, cataracts, or macular degeneration.
Furthermore, sunlight only appears during the day and cannot be present in spaces according to human needs. Therefore, artificial light—such as incandescent, halogen, and especially LED light (with advantages like diversity, environmental friendliness, meeting consumer tastes, and high luminous efficacy)—has emerged and gradually replaced sunlight for certain human requirements.
Light sources from lighting systems or electrical and electronic devices all have the potential to harm human health if not controlled.
When winter arrives, halogen lamps are used for heating. With very high power and intensity, coupled with proximity to the user, IRA rays can penetrate through the cornea and lens to the retina. After a sufficiently long period of exposure at high intensity, this can cause diseases such as cataracts and macular degeneration. Most simply, we can see immediate effects on the skin: after a period of exposure, the skin can become dry and burnt.

Light emitted from devices such as televisions, phones, tablets, laptops… after a period of exposure can cause eye strain, dry eyes, and gradually lead to blurred vision and impaired eyesight. During exposure, a large amount of high-energy light (blue light) emitted from LED chips in the screens of phones, televisions, laptops… can easily penetrate the cornea and lens; they penetrate deep inside the eye and can cause damage to the retina. Besides the harm to the eyes, these light rays can also damage our skin. Dermatologist Murad, founder of the Murad cosmetic brand, has shared insights on this issue. According to him, spending 4 working days in front of a computer, 8 hours per day, is equivalent to exposure to intense sunlight for 20 minutes. In reality, with just 7 minutes of sun exposure, your skin can suffer from burns.
Besides light sources from bulbs such as halogen, fluorescent, and incandescent lamps… as LED technology continues to advance, we can see LED lights appearing with high density everywhere. With light rays such as blue light, UV, or IR emitted from LED chips, scientists are concerned about their impact on human health, especially the eyes and skin. Why do LED lights affect the health of the eyes and skin? Let’s clarify this issue with Phuc Gia Laboratory!
II. OVERVIEW OF PHOTOBIOLOGY
“Photobiology” is the study of the interaction of optical radiation with living organisms.
“Optical radiation” is defined as electromagnetic radiation with wavelengths ranging from 100 nm in the deep ultraviolet (UV) region to 1 mm in the far-infrared (IR) region. However, this range is often limited for practical purposes to 200-3000 nm because ultraviolet radiation in the wavelength band below 180nm (vacuum UV) is strongly absorbed by atmospheric oxygen, and the effects of low-energy photons in the far IR are negligible.
Because optical radiation is strongly absorbed in tissue, with penetration depths ranging from a few micrometers (µm) for UV rays to millimeters (mm) for IR, the skin and eyes of the human body are at the highest risk of exposure.
“Biological response to exposure” is the result of many energy transformation processes, broadly classified as photochemical interactions or thermal interactions.
While photochemical interactions dominate in the short wavelength range where photon energy is greatest, thermal interactions tend to dominate at the long wavelength end of the spectrum.
In photochemical interactions, light of a specific wavelength (and carrying energy) excites electrons in cellular molecules, leading to the breaking or reorganization of chemical bonds within them. This can have direct consequences for DNA, whereby base pairs bond together, creating disruptions in the DNA chain. Indirectly, it can create an excess of highly reactive free radicals. These substances can interact with DNA (to cause structural reorganization) and with other cells such as retinal photoreceptor cells (to cause impaired cellular function and cell death). More importantly, DNA damage, if not repaired in time, has the potential to give rise to cancers.
The mechanisms underlying thermal interactions involve the absorption of light which increases the temperature at the point of contact, leading to protein denaturation and thermal cell damage.
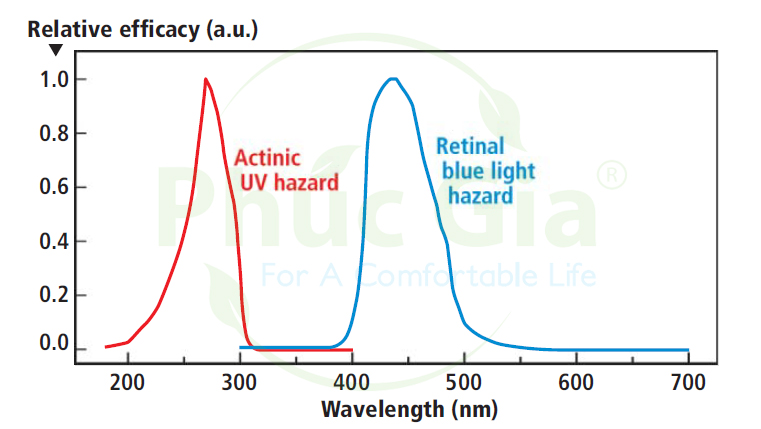
While thermal interactions pose an equal risk across all wavelengths, the strong wavelength dependence of photochemical interactions is characterized by hazard weighting functions (Figure 1). Such functions are the inverse of the dose (or energy) required at each wavelength to produce a certain level of response and are normalized to unity: “a low response requires a high dose and vice versa.”
Furthermore, while the effects of low-level thermal exposure can be mitigated by heat conduction away from the contact site, photochemical interactions generally follow the Bunsen-Roscoe law of reciprocity. This states that photochemical processes are dose-dependent, meaning that low-level, long-term exposure will cause similar damage as high-level, short-term exposure.
III. ANATOMY OF THE EYE AND PHOTOBIOLOGICAL EFFECTS FROM LIGHT WAVELENGTHS

The eye is composed of 11 main parts with functions as listed in the following table:
|
ORD |
EYE ANATOMY |
FUNCTIONS |
| 1 | Eyelids | Protects the eyes |
| 2 | Conjunctiva | Covers the eyeball, prevents infection |
| 3 | Sclera | Maintains the shape of the eye |
| 4 | Cornea | Focuses light |
| 5 | Iris | Adjusts the amount of light |
| 6 | Aqueous humor | Nourishes the cornea and the crystalline lens, maintains the shape of the cornea |
| 7 | Crystalline lens | Focuses light |
| 8 | Vitreous humor | Fills the space between the crystalline lens and the retina, maintains the shape of the eyeball |
| 9 | Choroid | Nourishes the eyeball |
| 10 | Retina | Light perception |
| 11 | Optic nerve | Connects the eye to the brain, transmits nerve signals |
Considering the photobiological effects of light wavelengths on the eye, we need to focus on the parts in direct contact with light: the cornea, pupil, crystalline lens, and retina. Let’s clarify the anatomy, role, and photobiological impact on these critical components of the eye with Phuc Gia Laboratory.
1. Cornea
The cornea (the “black of the eye”) is a thin, transparent tissue layer located at the front of the eyeball. It is the first part to come into contact with light, allowing light to pass through so the eye can see.
Characteristics: It is a transparent, very tough, and avascular (no blood vessels) membrane shaped like a spherical cap, occupying the front 1/5 of the eyeball’s outer shell. The diameter of the cornea is approximately 11 mm, with a radius of curvature of 7.7 mm. The corneal thickness at the center (average 520 µm) is thinner than at the periphery (average 700 µm). The curvature radius of the front surface of the cornea creates a converging power of about 48.8D, accounting for 2/3 of the total refractive power of the eyeball.
Anatomy: The cornea consists of 5 layers, from the outside in: Epithelium, Bowman’s membrane (also known as the “anterior elastic lamina”), Stroma (accounting for 90% of the corneal thickness), Descemet’s membrane (Bowman’s posterior elastic lamina), and Endothelium.

Function: The cornea acts like a lens with the function of controlling and focusing light rays into the eye. It accounts for 2/3 of the eyeball’s refractive power. To see clearly, light rays reaching the surface of the eyeball must be focused by the cornea and the crystalline lens to fall exactly on the retina. The retina converts light rays into nerve impulses transmitted to the brain, helping us perceive images. Additionally, the cornea acts like a filter that screens out harmful ultraviolet (UV) rays; otherwise, the crystalline lens and retina would be damaged by UV radiation.
Harmful effects of light rays (photobiological impact from light wavelengths) on the cornea
- UVC (100nm – 280nm): This is the ray with the highest radiation level and possesses a very high potential for significant harm to the eyes and skin.
- UVB (280nm – 315nm): UVB rays are almost entirely absorbed by the cornea, so they are not the primary cause of cataracts or macular degeneration; instead, they mainly cause corneal diseases such as keratitis, pinguecula, and pterygium.
- UVA (315nm – 400nm): UVA penetrates the cornea and enters the crystalline lens and retina; prolonged exposure will lead to macular degeneration or cataracts.
- Blue Light (HEV) (400nm – 500nm): Easily penetrates the cornea and lens, reaching deep inside the eye and potentially causing damage to the retina. Blue light has a short wavelength and carries high energy; therefore, as it passes through the cornea, it damages retinal cells. Long-term exposure leads to macular degeneration or cataracts.
- Infrared Radiation (780nm – 3000nm): When the cornea is exposed to infrared radiation exceeding regulated limits for a certain period, the overheating thermal reaction can cause corneal burns.
=> In IEC 62471, the photobiological impacts on the cornea are evaluated through exposure limits such as:
– ES (200-400nm): Photochemical UV hazard exposure limit for skin and eyes – causes corneal diseases such as keratitis and cataracts.
– EB và LB (300 – 700nm): Blue light hazard exposure limit for the retina – causes eye inflammation.
– EIR (780-3000nm): Infrared radiation hazard exposure limit for the eyes – causes corneal burns.
2. Iris – Pupil
The Iris: The pigmented ring surrounding the pupil that determines eye color (black, brown, blue, etc.).
The Pupil: The small black aperture located at the center of the iris that allows light to pass through and reach the retina.
Pupil Size: The size of the pupil depends on age and light conditions. Typically, the pupil ranges from 2mm to 7mm.
– Maximum pupil diameter: 7mm – at very low luminance (< 0.01 cd.m-2);
– Minimum pupil diameter: 2mm – at low luminance (< 10000 cd.m-2).
– The radiation flux entering the eye and absorbed by the retina (380nm – 1400nm) is directly proportional to the area of the pupil.
Function: The pupil can constrict or dilate thanks to the muscles within the iris to regulate the amount of light entering the eye. The less light reaching the eye, the more the pupil dilates, and vice versa.
=> Application of pupil aperture or size in IEC 62471:
– When the luminance of the light source is sufficiently high (> 10 cd.m-2), with an exposure time > 0.25s: an automated measurement aperture corresponding to a 3mm pupil diameter (area of 7mm2) is used to determine exposure limits;
– When the luminance of the light source is low, meaning there is little to no visible light while evaluating infrared radiation, the photobiological hazard exposure limits are assessed at a measurement aperture corresponding to a 7mm pupil diameter.
– For cases involving near-infrared sources, to evaluate photobiological hazards, exposure values are measured based on the assumption of a 3mm pupil diameter.
3. Crystalline Lens

Characteristics: The crystalline lens is transparent and located behind the iris.
Anatomy: The crystalline lens is composed primarily of water and protein. These proteins are arranged in an orderly fashion to allow light to pass through and focus on the retina. In some cases, proteins clump together, causing light passing through to scatter, creating opaque areas in the lens that block light from reaching the retina and reduce vision. This condition is called a cataract.
Function: It acts as a converging lens for light to pass through, focusing light rays exactly on the retina to create sharp images, helping us see both near and far. The lens must be transparent to create clear images.
Harmful effects of light rays (photobiological impact from light wavelengths) on the crystalline lens:
– UVA (315nm – 400nm): UVA can penetrate the cornea and enter the crystalline lens and retina; if exposed for too long, it will lead to macular degeneration or cataracts.
– Bluelight (HEV) (400nm – 500nm): Easily penetrates the cornea and crystalline lens. Prolonged exposure to the lens will lead to cataracts.
– IR rays (700-1400 nm range, highest risk potentially within 900-1000 nm): As we can see, IRA rays penetrate the lens, and IRB can penetrate the cornea to reach the lens; here, a photothermal effect causes protein denaturation at the point of contact or a photochemical reaction causes cataracts leading to decreased vision. Thermal interaction can affect the functionality of proteins and also lead to cellular damage. Some hypotheses suggest that cataracts caused by infrared rays may also be a photochemical reaction. As we know, there are currently conditions such as “Infrared Cataract,” also known as “industrial heat cataract,” “furnace worker’s cataract,” or “glassblower’s cataract.” Cataracts usually occur after many years of frequent high-level exposure; the duration depends on the difference between the exposure level and the threshold, with intense exposures producing reactions in the shortest time.
=> In IEC 62471, the photobiological impacts on the crystalline lens are evaluated through exposure limits such as:
– ES ( 200-400nm): Photochemical UV hazard exposure limit for skin and eyes, causing diseases for the lens such as Cataracts.
– EUVA (315-400nm): Near-UV hazard exposure limit for the eye – causing Cataracts.
4. Retina – Macula
The retina is a membrane inside the back of the eye responsible for receiving light focused by the lens. The center of the retina is the macula (yellow spot), where visual cells are most sensitive, helping identify the content and sharpness of images. Through the retinal optic nerves, light energy is converted into vision signals and sent to the analysis center in the brain. In the brain, these signals are decoded to create the perceived image.
Anatomy: The retina has 10 cell layers: Pigment epithelium layer, rod and cone cell layer, internal limiting membrane, outer nuclear layer, outer plexiform layer, inner nuclear layer, inner plexiform layer, ganglion cell layer, nerve fiber layer, internal limiting membrane, and retinal layers. This includes two main layers of neurons:
– Photoreceptor cells: Mainly rod cells (very sensitive to light, allowing us to see objects in low-light conditions, helping with distance vision) and cone cells (conversely, requiring more light but allowing us to perceive very small details of the object we look at, ensuring focused vision on a point and helping distinguish different colors).
– The remaining layer is the ganglion cell layer, also known as the nerve ganglion.
Light entering the eye is received by photoreceptor cells and converted into visual signals through a chemical reaction that turns light energy into electrical energy, which is then transmitted to the nerve ganglion. These ganglion nerve fibers converge at the optic disc and form the optic nerve that goes up to the brain.
| ORD | Photoreceptors | Light sensitivity | Acuity | Dark adaptation | Color vision |
| 1 | Rod cells | Low threshold | Low acuity | Late adaptation |
No (only distinguishes between white and black) |
| Extremely sensitive to low-intensity light; therefore, they play a crucial role in peripheral vision, low-light vision, as well as night vision. | Not present in the fovea (yellow spot) | ||||
| Function well in dark areas, allowing for night vision. | The loss of rod cells causes night blindness | ||||
| 2 | Cone cells | High threshold | High acuity | Early adaptation |
Yes There are 3 types of cone cells:
|
Additionally, the “Retinal Pigment Epithelium (RPE)” also constitutes an essential part of the retina: helping to nourish and protect rod and cone cells from the harmful effects of ultraviolet (UV) rays and blue light that damage the retina. The pigment epithelial layer also plays a role in preventing light reflection within the entire eyeball (as reflection would lead to blurred and unclear images).
Harmful effects of light rays (photobiological effects from light wavelengths) on the retina:
- UVC (100-280nm): This radiation has the highest energy level and possesses a very high potential for harm to the eyes and skin.
- UVA (315nm – 400nm): UVA penetrates the cornea, entering the lens and retina; prolonged exposure leads to macular degeneration or cataracts.
- Blue Light (HEV) (400nm – 500nm): Easily penetrates the cornea and lens, reaching deep inside the eye and potentially causing retinal damage. Blue light has short wavelengths and high energy levels; thus, as it passes through the cornea, it damages retinal cells. Long-term exposure leads to macular degeneration, cataracts, or more visible refractive errors such as myopia, vision impairment, dry eyes, eye strain, eye pain, and difficulty concentrating.
- Infrared Radiation (780-3000nm): IRA rays penetrate the cornea and lens to reach the retina, where thermal or photochemical reactions occur, leading to symptoms such as eye pain, corneal opacity, dry eyes, or macular degeneration.
=> In IEC 62471, photobiological effects on the eye are assessed through exposure limits such as:
– ES (200-400nm): Actinic UV hazard exposure limit for the skin and eye.
– EUVA (315-400nm): Near-UV hazard exposure limit for the eye.
– EB (300–700nm): Retinal blue light hazard exposure limit – small source.
– EIR (780-3000nm): Infrared radiation hazard exposure limit for the eye.
– LB (300-700nm): Retinal blue light hazard exposure limit.
– LR (380-1400nm): Retinal thermal hazard exposure limit.
– LIR (780-1400nm): Retinal thermal hazard exposure limit – weak visual stimulus.
IV. SKIN STRUCTURE AND PHOTOBIOLOGICAL EFFECTS FROM LIGHT WAVELENGTHS.
When the skin is exposed, part of the incident light is reflected, while the rest is transmitted through the epidermis and dermis, affecting the skin structure. Under photochemical effects (especially ultraviolet rays), they can cause effects such as erythema, skin cancer, aging, and melanogenesis.
Let’s explore the structure of the skin and the photobiological influences on it!
As an ever-changing organ, the skin consists of 3 main layers – epidermis, dermis, and subcutaneous tissue:
1. Epidermis
The epidermis is the outermost layer of skin that we can see and touch; it functions to protect the body against environmental impacts harmful to the body such as toxins and bacteria. It consists of 5 cell layers: Basal layer, Prickle cell layer, Granular layer, Clear layer, and Horny layer.
Cells in the horny layer are bonded together by epidermal lipids. These lipids are crucial for healthy skin: they create a protective barrier and retain skin moisture. The epidermis is covered by an emulsion of water and lipids (fats) known as the hydrolipid film. This film helps maintain sweat and sebum secretion, keeping the skin softer and acting as a barrier against bacteria and fungi.
=> Under the influence of radiation (the main culprit being ultraviolet radiation), the lipid layer in the epidermis can be damaged, impairing cell membrane functions: changing membrane permeability and reducing the conduction speed of nerve impulses. Damage to mitochondrial membranes affects ATP synthesis, and damage to lysosomal membranes causes a massive release of proteolytic enzymes within the cell. These impacts cause the skin to lose water, becoming drier, tighter, and rougher, losing skin cohesion and allowing bacteria to easily penetrate and create inflammatory reactions.
2. Dermis (or connective vascular tissue layer)
The dermis consists of a thick layer above the subcutaneous tissue and a wavy layer beneath the epidermis. The dermis is thick, elastic, and is the middle layer of the skin, comprising 2 layers: the papillary layer and the reticular layer.
The main structural components of the dermis are collagen fibers, elastic fibers, and connective tissues – which provide the skin with strength and flexibility, bringing a more youthful appearance. These structures are tightly bound with a gel-like substance (containing hyaluronic acid), which has a high capacity for binding water molecules to help maintain skin volume.
=> Optical radiation can produce free radicals that attack cellular structures, breaking down the skin’s collagen structure or even altering DNA. Collagen fiber structures can also be disrupted, causing a loss of skin elasticity, leading to wrinkles and aging.
3. Subcutaneous tissue (or subcutaneous fat layer)
The innermost layer of skin is where the body’s energy is produced, while also acting as a cushion and insulation for the body. It includes: fat cells, specialized collagen fibers (called tissue septa or boundaries), and blood vessels.
When optical radiation strikes the skin, depending on the distance and the intensity of the irradiation, radiant energy is transferred directly or indirectly to molecules, potentially breaking chemical bonds or dissociating biological molecules, causing the loss of their biological properties.
V. PHOTOBIOLOGICAL REACTIONS AND POTENTIAL HAZARDS RELATED TO LED LIGHTING
As LED technology and efficiency continue to evolve, there are growing concerns regarding the optical radiation produced by LEDs and potential exposure risks to humans.
Optical radiation includes radiations of the electromagnetic spectrum including ultraviolet radiation, visible radiation, and infrared (IR) radiation (200-3000nm as defined in photobiological safety standards), and exposure to optical radiation is associated with several reactions belonging to photobiological responses. These effects, including photochemical and thermal interactions, pose risks to human cellular tissue, particularly for the skin and eyes.
Photochemical interaction is typically a chemical reaction to ultraviolet light, in which bonds between electrons in cellular molecules are broken or rearranged. These cellular changes can lead to the impairment or destruction of functional cells.
On the other hand, thermal interactions are usually caused by the absorption of IR infrared radiation, generating high temperatures at the point of contact. Thermal interactions can affect protein functionality and also lead to cellular damage.
It should be noted that: photochemical reactions do not only occur in the ultraviolet region, just as thermal reactions do not only occur in the infrared region.
In humans, exposure to photobiological reactions of light from LEDs primarily affects the skin as well as the front surface of the eye and the retina.
When considering the hazards posed to the skin and eyes, three exposure scenarios must be taken into account: skin exposure, the front surface of the eye (cornea, conjunctiva, and lens), and the retina.

VI. EFFECTS ON THE SKIN
When the skin is exposed, a part of the incident light is reflected, the rest is transmitted through the epidermis and dermis. The main concern for the skin is due to exposure to ultraviolet rays, causing photochemical risks due to direct DNA damage, creating familiar inflammatory reactions such as erythema (sunburn).
Ultraviolet erythema – This photochemical reaction produces skin reddening, similar to sunburn and is the result of exposure to ultraviolet light (200-320 nm, peak 295 nm).
The harmful effects of light on the skin basically appear in the wavelength range of ultraviolet rays:
Example: erythema, skin cancer, aging, melanogenesis, etc. (IESNA 2010).
Another risk is the production of free radicals that can attack and transform DNA and other skin cells, such as collagen. Collagen provides the skin with elasticity, and damage to collagen will cause the skin to decrease elasticity, leading to the appearance of wrinkles and skin aging.
The risk of thermal burns also exists, but is of less concern because exposure is usually limited due to the accompanying sensation of pain at high temperatures. Besides, with repeated exposure to UV rays, the skin can increase melanin production to block the harmful effects of ultraviolet rays on the skin.
With visible light and infrared rays, burns can be caused by very high radiation. LEDs used in SSL are currently far from reaching the high radiation levels necessary to burn the skin. Therefore, the general population should not be worried about potential risks to the skin arising from the use of LEDs in lighting.

Only a small number of people with photosensitivity syndrome may see their pre-existing condition exacerbated by the blue light emitted from activated LEDs. Patients taking photosensitizing medications should also be aware of potential risks.
VII. EFFECTS ON THE EYE
The exposure of the superficial structures of the eye exhibits reactions similar to those of the skin.
The primary concern is in the UV region, which can lead to photokeratitis. This is an inflammatory photochemical reaction, similar to sunburn, occurring in the cornea and conjunctiva.
Photokeratitis is a photochemical reaction affecting the cornea of the eye and is caused by exposure to ultraviolet light (typically 200-320 nanometers (nm), Peak 270 nm). Symptoms are similar to irritation caused by sand or dirt in the eye.
Another possible result is cataracts caused by ultraviolet rays.
As the name implies, UV cataract is a photochemical reaction affecting the lens of the eye, resulting from exposure to ultraviolet light (290-325 nm, peak 305 nm). Blurred vision is a typical symptom.
In the IR range, a thermal reaction from chronic exposure to high levels can cause infrared cataracts.
Infrared cataract is a reaction to infrared light (anywhere from 700-1400 nm, peaks can be in the 900-1000 nm range) that affects the lens of the eye and leads to vision impairment. It is thought to be a photothermal effect but may also be a photochemical reaction.
Due to the transmission properties of the lens, retinal exposure only needs to be considered over the 300-1400 nm wavelength band. The exception is in the specific case of the aphakic eye, where the lens has not developed or has been removed during surgery.
The primary damage mechanism for exposure times greater than 10 seconds is the photochemical blue light hazard (photodermatitis), leading to the production of free radicals that damage both the photoreceptors and the retinal pigment epithelium (RPE – a layer of cells on the outer surface of the retina that supports photoreceptor function).
In shorter durations, the thermal hazard predominates, causing the denaturation of proteins and critical biological components of the retina.
Lasers and LEDs cause thermal effects by heating proportional to the power density of the radiation, which can lead to retinal tissue damage. Radiation with shorter wavelengths causes photochemical effects in the retina, altering the chemical properties of cells, and has dual limits (thermal and photochemical) in IEC 60825-1 between 400 and 600 nm. At shorter wavelengths below 400 nm, UV rays are largely absorbed and can cause damage to the cornea or possibly the lens. The eye has only a few protective mechanisms to respond to visual stimuli (380-780 nm). These include protective reflexes (blinking, pupil constriction, or head movement to limit the amount of light reaching the retina) and continuous eye movements (saccades), ensuring that the same area of the retina is not continuously exposed.
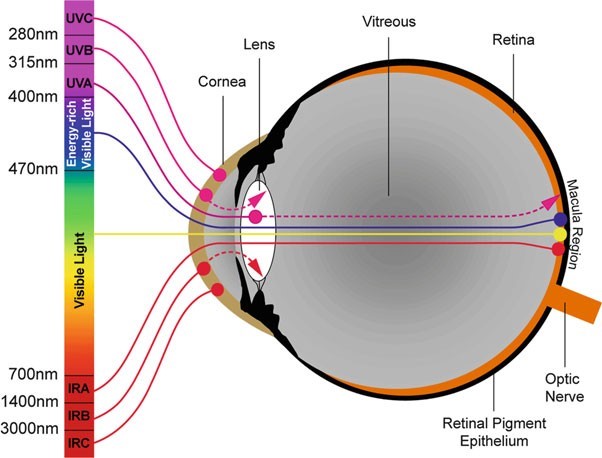
Depending on the wavelength band, optical radiation interacts with different eye tissues, as illustrated in Figure 2. Since ultraviolet radiation is primarily absorbed by the cornea and lens, excessive exposure leads to photokeratitis, conjunctivitis, and cataracts. Infrared radiation with wavelengths greater than 1.4 μm is primarily absorbed by the cornea and can cause corneal burns. Emitting negligible amounts of UV and IR radiation, LEDs should not be expected to contribute to photokeratitis, conjunctivitis, and cataracts.
Visible light (0.38–0.78 μm) and near-infrared radiation (0.78–1.4 μm) are focused on the retina and can cause retinal damage when overexposed, which can be the result of thermal damage or photochemical damage:
- Thermal damage (thermal retinopathy) occurs during short-term exposure to very high radiation levels. The exposure levels required to produce thermal damage on the retina cannot be met by the light emitted from LEDs of current technologies.
- Photochemical damage (photochemical retinopathy) appears after a short period of high-intensity exposure or after a long period of exposure to lower light levels.
It is important to mention that the exposure of the retina to a light source depends on both the exposure time and the retinal irradiance (W/m2), where the retinal image of the light source is created by the optical system formed by the cornea and the lens.
Retinal irradiance is proportional to the radiance of the light source (W.m-2.sr‑1), the transmittance of the eye media, and the pupil diameter, and is inversely proportional to the effective focal length of the eye (see Figure 3). The exposure dose (J/m2) is the time integral of the retinal irradiance over the exposure duration.

From a photometric perspective, retinal irradiance and source radiance are independent of the viewing distance. The viewing distance only determines the size of the optical retinal image. However, the actual “physiological” retinal image is the result of image spreading caused by eye movements. The eye movement component on the physiological retinal image is more significant for small optical images (distant light sources) than for large images (light sources at close distances).

VIII. PHOTOCHEMICAL RETINAL DAMAGE
In humans, light interacts with several ocular tissues and types of retinal photoreceptors (cones and rods, optic nerve cells…) to send received signals to the retinal optic nerve network, which is connected directly to the brain via the optic nerves to help us perceive light, images, etc. However, besides the photoreceptors, the retinal pigment epithelium (RPE) also plays a significant part in this process.
The RPE is the outermost layer of the retina (Figure 4). It plays a crucial role in the phagocytosis of the outer segments of photoreceptors (helping to nourish and protect rod and cone cells against the harmful effects of ultraviolet and blue light that damage the retina) and the regeneration of visual pigments.
RPE cells contain melanin (a photoprotective pigment) and lipofuscin, a substance that accumulates with age and is associated with several retinal disorders such as age-related macular degeneration (ARMD).
Photobiological research has been conducted for over 50 years on the retinas of mammals (rats, mice, monkeys) to determine lesions caused by retinal light exposure measured by the retinal radiation dose. This body of research reveals that there can be two types of retinal damage processes caused by visible light (ICNIRP 2013):
Type 1: damage observed after 12 hours per day (long exposure) is the bleaching of retinal pigments, with the potential accumulation of toxins in the RPE.
The action spectrum of type 1 damage is very similar to the optical sensitivity of the eye V (λ).
Type 2: damage is photochemical toxicity that induces reactions in the RPE after acute exposure to blue light.
Blue light stimulates lipofuscin by generating reactive oxygen species and free radicals, causing oxidative stress to RPE cells.
The existence of type 1 retinal damage was questioned by Van Norren in 2011 (Van Norren and Gorgels 2011), after an extensive evaluation of the literature and a lack of reproducible data regarding this type of damage. Figure 5 is an excerpt from Van Norren and Gorgels (2011). The graph summarizes the obtained doses for retinal damage as a function of wavelength.
Type 2 damage was first recorded in humans in the 1960s as the main cause of eye inflammation for arc welders and solar eclipse observers without eye protection (ICNIRP 2013). Research is currently being conducted to investigate the dose and wavelength dependence of light-induced retinal damage.
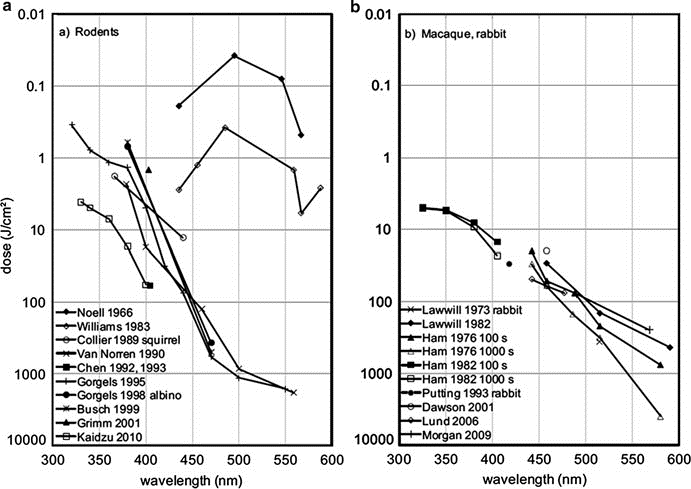
Figure 5. Dosage for retinal damage as a function of wavelength.
(a) Data for rats, unless otherwise specified.
(b) Data for macaques, unless otherwise specified.
IX. BLUE LIGHT HAZARD
Unlike Type 1 damage, Type 2 damage is quite well established and serves as the basis for ICNIRP guidelines regarding blue light hazards. For the general population, the action spectrum for blue light hazard is B (λ), represented in the chart below.
Image 10 – Action spectra for blue light hazard with a lens (phakic) B (λ), without a lens (aphakic) A (λ), and thermal-induced hazard spectrum R (λ).
However, individuals born without a lens (aphakic) or who have received a lens transplant (pseudophakic) are exposed to a greater amount of retinal UV and blue light compared to phakic subjects (phakic surgery aims to eliminate the need for nearsightedness glasses by inserting a very small lens between the iris and the natural lens) when exposed to the same light source.
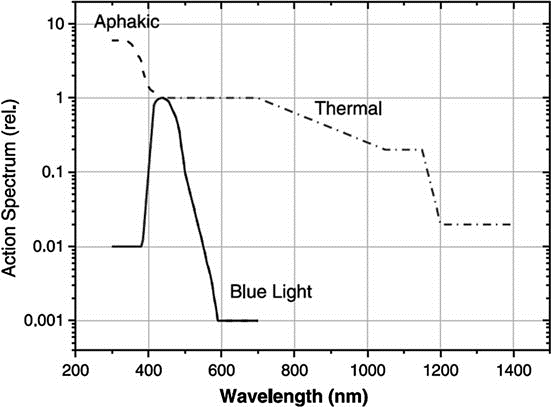
In these cases, the ICNIRP action spectrum is A (λ), also presented in Figure 6. ICNIRP also recommends using the A (λ) action spectrum when evaluating the photobiological safety of infants under two years of age, due to the higher transparency of their lenses compared to those of adults.
VI. PHOTOBIOLOGICAL SAFETY STANDARDS FOR LIGHTING PRODUCTS
The photobiological safety of lamps and lamp systems, such as luminaires and lighting modules, has been addressed internationally by the International Commission on Illumination (CIE), the Illuminating Engineering Society of North America (IESNA), and the International Electrotechnical Commission (IEC) through close cooperation and joint working groups. They resulted in the following standards describing the photobiological safety of lamps and lamp systems: joint publication CIE S009 (CIE 2006) and IEC 62471: 2006 (IEC 2006), and the IESNA / ANSI RP-27 series (IESNA 2000, 2005, 2007).
GENERAL PHOTOBIOLOGICAL SAFETY STANDARD CIE S009 / IEC 62471: 2006
IEC 62471 is a testing and classification standard that provides a procedure for evaluating the relative photobiological safety of lamps, lamp systems, and other non-lamp optical radiation sources. This process consists of three basic stages:
1. Measurement of absolute radiance and irradiance levels
2. Comparison of effective (“weighted”) levels with exposure limits defined by the standard
3. Determination of the risk group to which a product is assigned based on the level of hazard to the skin and eyes.
This standard, relating to the photobiological safety of lamps and lamp systems, provides a system for classifying light sources into several risk groups. The standard considers all photobiological hazards listed by ICNIRP that can affect the skin and eyes (thermal and photochemical hazards) from ultraviolet to infrared wavelengths.
Guidance is provided for performing the physical measurements (irradiance and radiance) necessary to evaluate exposure levels produced by lighting products in a laboratory. The standard introduces the concept of risk groups depending on the maximum permissible exposure duration evaluated for each type of photobiological hazard:
-
Hazards related to actinic UV, hazards related to UV-A
-
Hazards related to blue light (retinal blue light hazard) and thermal hazards related to visible and infrared radiation.
OTHER PHOTOBIOLOGICAL SAFETY REQUIREMENTS
Typically, end products combine LEDs and other components (lenses, etc.) that produce optical radiation. Because IEC 62471 is a “horizontal” standard, it does not directly address production, labeling, or user safety requirements that may be integrated for end products including optical radiation-producing components. For end-product manufacturers, IEC/TR 62471-2 provides further guidance on the appropriate application of IEC 62471 safety requirements, particularly regarding issues related to installation and use of the end product. IEC/TR 62471-2 specifically addresses the following:
- Hazard Distance – IEC/TR 62471-2 defines hazard distance as the distance at which the expected exposure level equals the maximum effective radiation value that does not harm the end user.
- Labeling – IEC/TR 62471-2 recommends specific types of product labeling, including notices, cautions, and warnings, based on the IEC 62471 risk group of the component and the wavelength of the optical radiation.
- User Information – IEC/TR 62471-2 recommends including risk group information determined according to IEC 62471, including hazard distance, exposure hazard values, and instructions for safe use of the end product.
- Viewer-related Risks – IEC/TR 62471-2 classifies viewer-related risks into “short-term unintentional,” “short-term infrequent, occasional,” and “long-term intentional.” Viewer-related risks associated with the end product may differ from the IEC 62471 risk group assigned to a component.
- Maintenance Personnel Considerations – IEC/TR 62471-2 recommends that the overall photobiological risk of the end product should be based on the IEC 62471 risk group of the optical radiation-producing component.
RISK GROUPS
Once the irradiance and radiance have been compared with the limits defined in the standard, the hazard level of the product can be established. IEC 62471 uses the following categories to establish the overall risk level of the product:
- Group 0 (RG0) – Exempt – the product does not pose any photobiological hazard affecting human health.
- Group 1 (RG1) (Low Risk) – the product does not pose a photobiological hazard within the limits of normal behavioral exposure. Products are safe for most applications, except for very long exposures involving direct eye contact.
- Group 2 (RG2) (Moderate Risk) – the product does not pose a hazard due to aversion responses to very bright light sources or thermal discomfort. In practice, products often do not pose an optical risk if human protective reflexes limit exposure time or when actual exposure is not prolonged.
- Group 3 (RG3) (High Risk) – the product may pose a hazard even for short or momentary exposure. These products carry potential risks even for temporary exposure.
CONCLUSION
Blue light hazard is the only photobiological hazard currently requiring consideration in existing SSL technologies, with the exception of LEDs using UV-emitting semiconductor structures. Blue light hazard is associated with photochemical damage caused by blue and violet light on the retina. Blue light hazard is related to retinal blue light radiance. Due to the high radiance of LEDs, retinal radiance levels are potentially high and must be carefully considered.
In general, photochemical damage to the retina depends on the cumulative dose to which a person has been exposed, which can result from short high-intensity exposure but can also appear after repeated long-duration low-intensity exposure. Blue light is recognized as harmful to the retina due to cellular oxidative imbalance. Blue light is also suspected to be a risk factor for age-related macular degeneration (AMD). Retinal blue light exposure can be estimated according to ICNIRP guidelines. Retinal blue light exposure levels produced at a distance of 200 mm by blue LEDs and cold-white LEDs (6000K – 7000K) often exceed exposure limits after exposure ranging from a few seconds (for blue LEDs) to several dozen seconds (cold white LEDs). Therefore, the potential toxicity at short distances from these LED components cannot be ignored.
However, when increasing the viewing distance to over one meter, the maximum exposure duration quickly increases to several thousand seconds, or even tens of thousands of seconds. This very long exposure duration provides a reasonable safety margin to assert that there is virtually no possibility of retinal damage from blue light from LEDs at further viewing distances (applicable to household LEDs, and true at the time of writing). However, it will have a significant impact on LEDs in handheld devices such as Phones, Tablets, Laptops…
Certain uses and applications based on recessed LED lights or LEDs combined with converging lenses (collimators) are directly related to high potential retinal blue light exposure levels.
Examples (but not limited to):
-
Testing and adjustment of high-power blue and cold-white LEDs by operators in lighting manufacturing facilities and lighting installers.
-
Toys using LEDs. Children are subjects sensitive to retinal blue light exposure.
-
LED daytime running lights on cars when activated near children and other sensitive individuals (not within the scope of this appendix).
-
LEDs sold for household applications (consumer market) where the lamp may be viewed at short distances up to 200 mm.
For all SSL devices (LEDs, LED modules, LED lamps, LED luminaires, etc.), a blue light risk assessment must be performed. The primary tool is the IEC 62471 Standard. It provides a system for classifying light sources into several risk groups based on the maximum permissible exposure time evaluated at a certain viewing distance: Risk Group 0 or Exempt Group (no risk), Risk Group 1 (low risk), Risk Group 2 (moderate risk), and Risk Group 3 (high risk).
IEC 62471 has two different criteria for determining viewing distance. Light sources used in general lighting should be evaluated at a distance corresponding to an illuminance of 500 lux. Other types of light sources should be evaluated at a reference distance of 200 mm. For LED components that will be integrated into a higher-level product (e.g., phones, laptops, tablets, etc.), IEC 62471 requires the use of a 200 mm distance.
The choice of viewing distance in IEC 62471 is sometimes unclear and impractical under real use conditions. Technical report IEC TR 62778 published in 2012 clarified and addressed this ambiguity of IEC 62471 when applied to evaluate the blue light hazard of LEDs and SSL equipment. Following the guidelines of IEC TR 62778, LED manufacturers must report the risk group of their component (RG0, RG1, or RG2).
According to IEC TR 62778, it is sometimes possible to transfer the risk group of an LED to its integrated higher-level product. In the case of RG2 equipment, the manufacturer should provide the boundary between RG1 and RG2 with threshold illuminance and threshold distance, which can be considered a reasonable safety distance. RG2 products should be sold with clear information about the threshold distance. Otherwise, RG2 products must be labeled according to IEC TR 62471–2, to inform users “not to stare” at the operating lamp as it may harm the eyes.
For SSL products aimed at consumer applications (e.g., classic LED bulbs), the risk group should be limited to RG1 at 200 mm, which can be considered the shortest viewing distance encountered at home.
IEC 62471 does not take into account the sensitivity of specific population groups, which may be characterized by cumulative sensitivity to visible light:
-
People with pre-existing eye or skin conditions that artificial light may trigger or exacerbate.
-
Aphakics (those without a lens) and pseudophakics (those with an artificial lens), who therefore either cannot, or can only partially avoid certain short wavelengths (especially blue light).
-
Children because their skin and visual systems are immature.
-
The elderly because their skin and eyes are more sensitive to optical radiation.
Photobiological standards related to lighting systems should be expanded to cover children and aphakic or pseudophakic individuals, taking into account the corresponding phototoxicity curves published by ICNIRP in its guidelines. Certain types of workers are exposed to high doses of artificial light (long exposure times and/or high retinal radiance levels) in their daily activities (e.g., lighting professionals, stage artists, etc.).
Since damage mechanisms are still not fully understood, exposed workers should use appropriate personal protective equipment as a precaution (e.g., blue light blocking glasses).
New generations of white-light-emitting LEDs are currently being developed using violet and UV chips. This is the case for “GaN on GaN” LEDs currently incorporated in some commercial SSL products. Such devices are now quite popular due to the advantage of being able to create a continuous spectrum; however, the photobiological safety of these LEDs and products using them must be carefully evaluated because UV and blue light radiation may exist in the emission spectrum. Evaluation should also be conducted for blue light and ultraviolet hazards. Careful inspection of the aging of these products is necessary as the degradation of the phosphor compound that may occur could increase the emission level of short-wavelength light.
Compiled and Synthesized by: Mr. Le Thu Phuc Gia (Le Tuan Hieu) – Phuc Gia Laboratory
For more details, please contact us at:
PHUC GIA LABORATORY CORPORATION
PHUC GIA CERTIFICATION CENTER
PHUC GIA INSPECTION TESTING CENTER
Hotline: 0981 996 996/ 0982 996 696/ 024 7779 6696
E-mail: lab@phucgia.com.vn/cert@phucgia.com.vn/info@phucgia.com.vn
Website: phucgia.com.vn
Working time: Monday to Friday 8:00 – 18:30; Saturday 8:00 – 12:00

![QUOTATION – Testing and Other Certification Services [2026]](https://phucgia.com.vn/wp-content/uploads/2017/03/bao-gia-thu-nghiem-chung-nhan.png)